
Welcome to the blog of thelongevityproject.online, dedicated to graduate and postgraduate topics related to the physiology of aging I have written over the years, revised for ease of reading. My content is tailored for individuals 55 and over, providing unique insights on how proper lifestyle choices can mitigate the aging process. I encourage you to leave comments, contact me, and above all, become more educated on this vital topic.
I. Biomarkers Related to the Aging Process
As an individual ages, key biomarkers can be observed that contribute to the degradation and eventual demise of the organism. This degradation or dysfunction starts at an earlier age than overt symptoms are witnessed. What biomarkers start to degrade first depends on the lifestyle and genetics of the individual. Nevertheless, a vicious cycle generally will begin, with the various biomarkers and their dysfunction feeding off each other, hastening the organism’s decline. In the following research, I have chosen three biomarkers that are intimately connected, and in the real world, are surely most common.
Sarcopenia
The word “sarcopenia” is derived from two Greek words: the prefix “sark” translates to meat; the suffix “penia” translates to loss. (Bellanti, 2021). As an individual ages, less hormone secretion is occurring, such as decreased testosterone, growth hormone (GH), insulin-like growth factor (IGF-1), and estrogen. If a practice of strength training is not ongoing as one ages to mitigate this loss by stimulating protein synthesis, the potential for falls and injuries are very common. In fact, by the time individuals are over the age of 80, up to 50% of those individuals suffer from sarcopenia (Bellanti, 2021).
Essentially, 2 major things are happening during the process of sarcopenia: there is a loss in muscle quality first, followed by a loss in muscle quantity.
- In a loss in muscle quality, a loss in strength can be noticed due to key structural changes, such as a decrease in the number of nerve cells that signal muscles to move (a key factor), defective anabolic signaling of GH, a general decrease in the macronutrient (CHO, fat, and protein) uptake, and a replacement of muscle tissue with fat and fibrous tissue.
- Then later, in loss of muscle quantity, there is a decrease in both the number and size of muscle fibers.
A byproduct of one’s strength is power, and that power loss or velocity when doing repetitive tasks quickly is lost first to a greater degree than strength. Power needs an explosive anaerobic system for increased velocity (type II muscle fibers); unfortunately, there is a decrease in the number of working nerve cells that trigger that power, even in the early stages of sarcopenia.
But engaging in sensible practice of strength training regularly, focusing on movements that challenge mobility and functional strength that simulate to some degree activities of daily living (ADL), one can preserve strength, power and muscle mass. At least twice weekly is the current recommendation, with a 48-hour recuperation between those workouts (CDC, 2023)
Mitochondrial Dysfunction
So, strength and power are adversely affected, but what about aerobic endurance? Unfortunately, the aerobic system (types I and IIa muscle fibers) is adversely affected as well due to dysfunctional mitochondria caused by the aging process. This ultimately also leads to sarcopenia. In the healthy human, there is a delicate balance between mitochondrial biogenesis that creates new mitochondria, and mitophagy, the selective destruction of old or damaged mitochondria. However, physical inactivity in the aging individual causes greater mitochondrial mitophagy due to oxidative stress, thus upsetting the delicate homeostatic balance.
Yet even in the elderly, mitochondrial biogenesis can occur via the practice of regular aerobic activity, which activates key signaling pathways (A master regulator of mitochondrial biogenesis is called peroxisome proliferator-activated receptor gamma coactivator 1 alpha). (Bellanti, 2021). This begins a cascade of reactions leading to the production of proteins needed to synthesize new mitochondria. Aerobic activity that is at a conversational pace, but the individual is breaking a sweat (zone 2) seems to be the best intensity for mitochondrial biogenesis. (Marshall, 2024). The current recommendation is getting at least 150 minutes of cardiovascular exercise per week (CDC, 2023).
Diastolic Dysfunction
Through the natural process of aging, exacerbated primarily by long standing hypertension, as well as other co-morbidities, the Left Ventricle (LV) of the heart (the chamber that is responsible for delivering blood into systemic circulation) becomes stiff and less compliant. Essentially, concentric remodeling (scar tissue) occurs in the myocardium, caused by a rise in collagen within the extracellular matrix (Aurigemma, 2006). As a result, the preload, or amount of blood in the LV chamber prior to LV contraction or systole, is decreased. As a result of less blood leaving heart into systemic circulation with each heart beat, there is a decreased stroke volume, which translates into a decreased cardiac output (SV x HR/min = CO). A lower CO translates into a lower VO2max, or how much oxygen one’s working skeletal muscles can extract. This is known as diastolic dysfunction (DD), and it adversely affects an individual’s VO2max potential.
How can aerobic exercise mitigate DD?
Regular aerobic activity (not strength training) can reduce the stiffening of the heart muscle and thus improve the filling of the heart during diastole. In fact, aerobic training for three to four months can significantly improve VO2max, decrease symptoms of shortness of breath with exertion, and improve quality of life measures (Fogoros, 2024).
What looks good on paper versus the real world
On paper, regular practice of strength training and aerobic activity as one ages can potentially postpone one’s demise for a decade or more. In reality, not many individuals over the age of 65 are even close to practicing the minimum amount recommended to gain any benefit (CDC, 2023). In fact, only 8.2% of older adults met the criteria for both aerobic and strength training activity (Kruger, 2007). More recently (Pahor, 2014), this trend continues. In the LIFE Study randomized clinical trial, after completing the structured exercise program for sedentary individuals, there was a one year follow up. The physical activity group arm at this follow up had regressed to where the control group arm was regarding regular exercise, and the other arm of the study, the health education group, had at this point caught up to the physical activity group.
How can retention be improved
What is the defining difference between people who continually exercise at a high level, despite orthopedic or other insults to their body, compared with more sedentary individuals? The short answer is intrinsic motivation. Individuals who exercise day after day, one decade after another are generally motivated by the enjoyment of running, biking, swimming, walking, playing a sport. They may find personal growth through the process, as they feel stronger, healthier, more flexible, at ease. They may find enjoyment in setting personal goals to attain. They may find a sense of purpose or well-being from their chosen physical activity. In contrast, with extrinsic motivation, individuals may want to improve solely physical appearance. They may exercise for some reward, whether money, a vacation, a trophy.
How can an individual become more intrinsically motivated? I honestly do not have an answer. As a strength and conditioning specialist, I can only guide and educate, and from that, motivate them in a way that is more sustainable. Over the hundreds, perhaps thousands of individuals I have trained throughout my life, I have only worked with a small handful of individuals that were intrinsically motivated. Those individuals will always exercise, whether I am in the picture or not, whether they are injured or recovering from injury or not. I believe they appreciate my advice, guidance, creativity and intuition when working with them, but they could continue without me.
One key element of their workout week that looks different, day in and day out from extrinsically motivated people, is their consistent desire to do other forms of physical activity on the days that I do not see them, for a more comprehensive exercise program. After all, what I guide them through is but a drop in the bucket, and they realize that.
BB
II. Environmental Enrichment
According to Francisco Mora (Mora, 2007), environmental enrichment can help increase many factors in the brain of elderly organisms that are necessary to keep it youthful. One of the key factors that is stimulated through environmental enrichment and aerobic exercise is Brain Derived Neurotrophic Factor (BDNF), which enhances brain’s neuroplasticity by promoting synaptic plasticity, neurogenesis, and the actual survival of neurons. BDNF is like miracle-grow for the brain, according to Charles Duhigg (Duhigg, 2012). These structural restorations are crucial for learning, memory and mood (Marosi, 2013).
Neuroplasticity or neural plasticity is the brain’s ability to reorganize and restructure itself on a cellular level (Perry, 2021) as we adapt to changes through new experiences, new environmental exposure, and even brain damage. Confronting a new environmental challenge requires neural networks to alter themselves and generate new connections. Use it or lose it, as the saying goes.
There are many examples of cognitive enhancement that have been shown to improve neuroplasticity through various studies. For instance, the MRI comparison in individuals learning to juggle versus the control group showed an increase in size in key areas associated with the visual processing of movement (increased size in bilateral mid-temporal grey matter; left posterior intra-parietal sulcus). Similarly with London Taxi drivers versus the control group, the drivers showed greater growth and volume in the posterior hippocampus, important for spatial memory (Sage, 2014).
Further, Erickson and colleagues found that training which emphasized intellectual challenges like semantic elaboration during a memory encoding task led to improved performance in older subjects, functionally activating the pre-frontal cortex (Sage, 2014). This growth and development in the brain is due in large part to this reorganization and restructuring due to neuroplasticity.
But what about something more modern? Can present-day technology such as video games act as an equivalent function that would provide environmental enrichment, and thus stimulate neuroplasticity and improve hippocampal function in individuals naïve to gaming? At the University of California, Irvine, 39 self-described video gamers and 29 self-described non-video gamers were gathered for participation in a pilot study (Clemenson, 2015). The control group played no games; The active control group played a 2-D game (Angry Birds); and the experimental group played a 3-D game (Super Mario).
At the end of the study, the once naïve 3-D gamers had an increase in hippocampal stimulation, thus an enhancement in hippocampus-associated behavior due to playing a complex game requiring greater spatial aptitude than in 2-d games - or in any real-world environment because of obvious safety concerns.
Finally, can an old technology that has been around for centuries provide a similar amount of neuroplasticity stimulation? Yes. Even in older adults, learning to play the piano has been shown to improve neuroplasticity. Engaging in the challenge of sight reading a new piece, and refining skills to perfect that piece, promotes the growth of new neural connections (Xinyue, 2023). Further, piano playing has been linked to cognitive preservation, including improved memory and executive function in older adults. In fact, the structured nature of piano playing, along with its rhythmic and melodic attributes can facilitate motor recovery in individuals with a variety of neurological disorders, such as Parkinson’s disease and stroke. And, as a side effect, you learn lots of cool tunes and are a hit at holiday gatherings.
BB
III. Salt Sensitive Hypertension: A different Treatment Paradigm
In salt sensitive humans, Signal Transducer and Activator of Transcription 3 (STAT3) is the most critical transcription factor for upregulating the angiotensinogen (AGT) gene, which leads to elevated blood pressure.
There are several key upstream pathways that eventually converge to activate STAT3 in response to a high salt intake by ultimately activating the JAK-STAT pathway; then, downstream to STAT3, SMAD3 (Saleem, 2025) is activated (Sma from the nematode Caenorhabditis elegans, and Mad from the fruit fly Drosophila).
First, an overview:
In an individual who is not salt-sensitive, a high-salt intake normally suppresses the renin-angiotensin-aldosterone-system (RAAS) activity, leading to reduced renin and angiotensin II, and lower aldosterone levels. This leads to a negative feedback loop where the body’s response to salt intake is to suppress the hormones that raise blood pressure.
In an individual with salt-sensitive hypertension, Ang II can continue to activate the RAAS through a positive feedback loop involving the intrarenal formation of angiotensinogen, often driven by pro-inflammatory cytokines like IL-6. This leads to the activation of the JAK-STAT pathway, which further enhances Ang II production and signaling, independent of aldosterone levels.
Myeloid Antigen-Presenting Cells: they are cellular bridges between the innate and the adaptative immune systems because they contact a pathogen at the site of infection and communicate this encounter to T lymphocytes in the lymph node (Miao, 2022).
STAT3 and beyond:
- A high salt intake in salt-sensitive individuals leads to salt-sensitive hypertension by the release of renin from the juxtaglomerular cells (JG) in the kidney, which initiates RAAS inappropriately.
- Angiotensin II, a key hormone in the RAAS, directly increases inflammation by raising levels of pro-inflammatory cytokines, most notably interleukin-6 (IL-6) from activated myeloid cells, including myeloid antigen presenting cells (APCs), in turn, this upregulates the JAK-STAT pathway, through the Janus Kinases (JAKs), particularly JAK2 protein. Activated JAK2 phosphorylates STAT3 monomers. This all occurs in the cell cytoplasm.
- Downstream and enhanced by the JAK-STAT pathway, SMAD3, a member of the Transforming Growth Factor (TGF) signaling pathway, is activated
- Once activated, the SMAD3 complex is translocated to the cell nucleus, where it can then bind to the angiotensinogen (AGT) promoter to initiate transcription.
- Further downstream, activated SMAD3 results in increased production of pro-inflammatory molecules such as IL-6 in the kidneys, activating T-cells and raising blood pressure, thus contributing to hypertension and damage, locally in the kidneys, and systemically (Saleem, 2025).
Preventing the Damage by using Myeloid-Specific JAK2 inhibitors
- Use inhibitor therapy specific to myeloid cells, thus target the root cause of salt-induced inflammation in those with salt-sensitive hypertension.
- The inhibitor blocks the activity of JAK2, which then halts the entire downstream cascade.
- This prevents the activation of STAT3 and SMAD3, thus mitigating the production of pro-inflammatory molecules.
- The overall effect in salt sensitive individuals dampens the inflammatory response in endothelium and lowers the blood pressure (Saleem, 2025).
BB
IV. Young Blood
When a variety of species voluntarily exercise aerobically, certain enzymes are released that can reverse the brain’s aging process, specifically by reestablishing neurogenesis in the brain’s hippocampus. For instance, plasma concentrations of glycosylphosphatidylinositol (GPI)-specific phospholipase D1 (Gpld1), a GPI degrading enzyme derived from the liver, are released during aerobic activity that do just that. If this enzyme could somehow be transplanted into sedentary mice from aerobically fit and active mice, it could, in theory, improve cognitive function in sedentary mice (Horowitz, 2020). If effective, could this then be duplicated in humans with consistently positive results on cognition? Would this help with diseases like Alzheimer’s? If results were encouraging, how often would this installment need to be done? Would there be ethical concerns if there were dramatic improvements at first, only to lead to the eventual regression and demise of the individual?
Preclinically with animal models, when Gpld1 and other important factors released during exercise such as brain derived neurotrophic factor (BDNF) were transferred from young mice to elderly mice, either by heterochronic parabiosis (where the circulatory systems of young and old are joined), or administration of young plasma to elder mice, improvements in cognition and increases in neurogenesis (confirmed by expression of the key markers BrdU and NeuN showing key neuronal growth in dentate gyrus of hippocampus) in the aged hippocampus were observed (Horowitz, 2020). Parabiosis has been utilized in animal studies for decades. Plasma injections are a more recent delivery system, which is simpler in its delivery system.
How does this translate to humans? It has been shown through numerous studies that consistent aerobic activity throughout life mitigates cognitive decline and improves cognition in populations at risk for Alzheimer’s disease (Dhahbi, 2025). But for elderly individuals that cannot reap the benefits of aerobic activity due to a variety of orthopedic and metabolic reasons, can the transfer of those key enzymes and factors be transferred over as was done in the preclinical setting? As of now the results are mixed.
Clinically, there is no evidence according to neuroscientist Tony Wyss-Coray of Stanford University in Palo Alto, California, who was principal scientist in the 2014 study in mice (Kaiser, 2016). Plasma injections from young blood to old blood in humans, nor parabiosis seem to have that positive effect that it did with mice. In Ambrosia’s clinical trial, 600 people over 35 receive 1.5 liters over 2 days of a plasma injection from a donor under 25. Pre and post blood tests compare more than 100 biomarkers that vary with age. The results are analyzed. The cost is 8,000$.
In contrast, most platelet rich plasma injections cost on average 1,000$ (Boston concierge orthopedics, 2025). Further, in most trials there is a placebo arm. In the Ambrosia trial, there is none. Thus, profits are ahead of actual improvements. But based on Wyss-Coray’s research and hypothesis that young blood injected into old could have benefit, a study was done in individuals with mild to moderate Alzheimer’s disease. The results were modest, showing its safe effect on humans, with mild improvements in memory (Goldman, 2018). If the intricacies of this model of treatment eventually get perfected where results are remarkable, then regular supplemental injection or infusion would have to be ongoing; otherwise, the individual will regress back to the less vibrant self.
This reminds me of the book called Flowers for Algernon (which was eventually made into a movie). In the book, researchers have found, through invasive laboratory tests, a way to make mice much smarter than normal, and therefore more complex mazes would have to be designed to heighten the intellectual challenge in order to develop new neural pathways. After successfully completing their first experiment on the first mouse called Algernon, it was decided to try the same procedure on Charly, a human with mental retardation, but with a strong desire to learn. Thus, in theory, the final results could potentially be very stark in contrast to the start.
Charly’s initial IQ was 68 before the surgery, rising to a peak of 185, several weeks post operation - after weeks of nurturing new neuronal growth with challenging intellectual stimulation. The story, told through Charly’s personal progress reports, shows how in the beginning his sentence structures were very basic with many grammatical errors; this is contrasted with his journaling several weeks out, where the sentence structures are quite complex with physiological and biochemical data beyond the scope of most scientists. This unfortunately is followed by first the regression of Algernon the mouse, and then Charly, who is quite aware of his fate at that point, and his struggle to develop new interventions that would reverse the regression. Thus, ethical questions come into the story, as well as the complex, emotional toll, which could hit home in a real-world scenario.
BB
V. Stem Cell Regeneration
Stem cells are crucial for longevity because they can regenerate and repair tissue throughout life, containing the all-important chromosomes that in turn contain genetic instructions for that cell. Thus, they are the body’s internal repair system, continuously replacing damaged or lost cells to maintain the function of organs and tissues on a more macro level. But stem cell function declines or deteriorates as we age, impacting their ability to self-renew and differentiate properly. This decline and deterioration are linked to shortened telomeres, which are the protective caps on chromosomes that are lengthened by the enzyme telomerase. This enzyme expression is expressed by stem cells to enable more divisions. However, the stem cells become shorter with each division, eventually not being able to divide. This process is called replicative senescence (Pizzul, 2023).
There are many different types of stem cells in the body, depending on their function. For instance, mesenchymal stem cells are vital for bone and muscle; neural stem cells are crucial for brain health; hematopoietic stem cells (HSC) on the other hand are crucial to producing blood and immune cells, which are constantly needed to maintain the body’s health. HSCs divide an average of 56 times over a person’s lifetime, with roughly half of these divisions occurring within the first 24 years of life. As individuals age, adult stem cells like HSCs divide less frequently, with an average of less than one division every two years (Life Sciences, 2025).
According to Oh, et al (Oh, 2024), there are several key strategies that can be used in theory to address aged stem cells: using senolytic compounds that can induce the removal of senescent cells from aged tissues (quercetin and disatinib), or senomorphics that reduce the expression of senescent-associated genes and inflammatory factors without actually killing the senescent cells; targeting molecular pathways that become perturbed during aging, such as those involved in DNA damage, repair, and reactive oxygen species (ROS) production, by developing interventions; and utilizing caloric restriction in order to improve stem cell function, potentially enhancing stem cell proliferation and function. I will explore a couple of these potential avenues that could prevent or at least mitigate the stem cell from going down that path towards senescence and the corresponding inflammation to tissues.
Reactive Oxygen Species
There is a longstanding notion that an increase in ROS may drive stem cell dysfunction with age. According to Denham Harman, “accumulated cellular damage and declining mitochondrial integrity in aged cells leads to elevated ROS production, which in turn drives a vicious cycle that further damages cellular macromolecules and disrupts mitochondrial oxidative phosphorylation, leading to eventual cellular decomposition.” (Harman, 1972).
The pathway perturbed by ROS are the DNA damage response (DDR) pathway, leading to cell cycle arrest via the p53/p21 and p16/pRB pathways, and the MAPK pathway. The cascade of events starts with damage to DNA caused by ROS, which activates the DNA damage response (DDR) pathway; this pathway in turn activates cell cycle arrest through the p54/p21 and/or the p16/pRB pathways. Further, the MAPK pathway is also required for the activation of senescence in response to ROS (Oh, 2014).
Therapies such as N-Acetyl Cysteine (NAC) have been shown to reduce ROS levels and DNA damage. In fact, it has been shown preclinically and clinically to exhibit antioxidant, anti-infective, and anti-inflammatory activity, and its use as a mucolytic is well established (Santus, 2024). NAC was first introduced in 1965 for its role in breaking up mucus, thus helping in the treatment of acute bronchitis, chronic obstructive pulmonary disease (COPD), bronchiectasis, and cystic fibrosis. Oxidative stress and inflammation contribute to the development of these pathologies. NAC’s mechanism in pulmonary conditions involves the inhibition of the activation of NF-kB and neurokinin A production, resulting in a reduction in interleukin-6 production, which is a cytokine present in the sputum and breath condensate of patients with COPD.
NAC’s shielding effect against ROS may be attributed to its function as a precursor to reduced glutathione (GSH). NAC is a synthetic source of amino acid cysteine, which is a building block for GSH; thus, NAC helps replenish the body’s stores of glutathione. GSH is important because it directly scavenges various ROS, such as hydrogen peroxide and superoxide anions, and is a crucial co-factor for antioxidant enzymes like glutathione peroxidases (GPx). These enzymes convert toxic peroxides into non-toxic water and alcohols (Santus, 2024).
Under normal conditions, ROS act as important signaling molecules for normal physiological activities. The GSH/ROS balance ensures proper cell signaling. Under severe stress for instance, where ROS production overwhelms the antioxidant capacity of GSH, oxidative stress can occur, which can damage cellular components such as DNA, proteins, lipids, and lead to cell apoptosis. GSH’s chronic depletion is implicated in various diseases, including neurodegenerative disorders and cancer (Liu, 2022).
However, before reaching for the NAC bottle, it should be known that using synthetic NAC can have negative effects, particularly at high concentrations, or with long-term use, as it may disrupt the essential balance of ROS that is required for proper stem cell differentiation and signaling. For instance, studies have found that while moderate ROS scavenging can enhance certain stem cell functions, complete ROS scavenging using NAC can completely inhibit the differentiation of some stem cells, such as human embryonic stem cells into vascular embryonic progenitor cells. Thus, a minimal, physiological level of ROS is necessary for normal stem cell development and differentiation (Zheng, 2024).
Mitochondrial Dysfunction
Although the free radical theory of aging points to elevated ROS as a principal cause of mitochondrial DNA (mtDNA) mutation according to Oh, et al, (Oh, 2014), there is a more efficacious and safe way to improve mitochondrial function and therefore stem cell health without the use of supplements such as NAC that have a small window for safety and efficacy. According to Cerletti, et al (Cerletti, 2012), caloric restriction leads to a greater number of mitochondria in muscle stem cells. Because stem cells adapt to lower calorie states by shifting their metabolism from glycolysis to oxidative phosphorylation, mitochondrial function and efficiency is improved. CR also modulates key signaling pathways like mTOR1, and sirtuin activation. For instance, CR dampens the activity of the mTOR1 pathway, which is a key nutrient sensor. The regulation of mTOR1 pathway is crucial for maintaining stem cell quiescence and self-renewal and preventing their premature differentiation and exhaustion. On the other hand, CR activates sirtuin enzymes such as SIRT1, which promotes mitochondrial biogenesis and function via activation of PGC-1a and FOXO, further linking mitochondrial health to stem cell function (Kadharusman, 2021)
In conclusion, some organisms such as the lobster have telomerase active in most of their cells for life, allowing them to maintain telomere length in most cells and avoid the limitations of cell division that lead to aging. Thus, they could have a potentially indefinite lifespan. Unfortunately, the molting process they undergo, particularly in later years, seems to be their downfall, as it takes tremendous amounts of energy to undertake the molting process and then the regrowth of a new shell (Berthold, 2025). But a greater span of telomerase activity in humans would potentially precipitate greater potential for cancer development. Perhaps if we better understood why some ethnicities do not show a decline in telomere length with age compared with controls, we could better understand genetic factors and potentially change them through epigenetic means. There is a correlation between Ashkenazi Jewish centenarians and their telomere length and lipid profiles compared with controls. In the same association analysis, it was shown that individuals with hypertension, metabolic syndrome, or diabetes had shorter telomere lengths compared with subjects without these disorders. Correcting this genetic deficit may prove advantageous (Atzmon, 2009).
BB
VI. Enhancing an Important Biomarker Measurement of Aging with AI
There are presently 12 hallmarks of aging: Genomic instability, telomere attrition, epigenetic alterations, loss of proteostasis, disabled macroautophagy, deregulated nutrient-sensing, mitochondrial dysfunction, cellular senescence, stem cell exhaustion, altered intercellular communication, chronic inflammation, and dysbiosis. When these 12, interconnected hallmarks are all able to be addressed, aging can halt and longevity can occur (Regenerative Medicine, 2025), in theory. But many of these interconnected processes are not fully understood, which is a problem, because not just a few of these hallmarks, but all 12 need to be addressed to stave off ageing. Maybe more. There probably are more hallmarks yet to be discovered. According to Keshavarz, et al (Keshavarz, 2022), despite the framework’s usefulness, there are weaknesses that prevent strong conclusions about its application.
Associated with some of these hallmarks are measurable indicators of age-related degeneration called biomarkers, biological measurements that can be quantified and reflect an individual’s true biological age and not chronological age. As a result, these powerful biomarkers can provide better insight into how an individual is aging. VO2max, or maximal oxygen uptake, is one of those more powerful biomarkers because VO2max is the single best predictor of cardiorespiratory fitness available. It is also inversely associated with all-cause mortality and chronic disease like heart disease and diabetes (Christian, 2025).
One of the key reasons why the VO2max measure is so powerful is because it provides so much information, acting as an integrated measure of the entire “oxygen chain”, from an individual’s heart to their lungs, blood vessels to their muscle cells, transporting and utilizing oxygen during intense exercise (Pnoe, 2025). If any links in this chain are adversely affected, VO2max will be compromised. If, for instance, the left side of the heart is adversely affected (Left atrium, ventricle, or their valves), cardiac output could be affected; likewise, if the right side of the heart is affected (right atrium, ventricle, their valves, or lungs), cardiac output could also be affected; and if an individual is in a weakened state due to lack of muscular strength or sarcopenia, or there is a chronic orthopedic injury, this too can put a kink in the “oxygen chain”, lowering an individual’s VO2max score.
Today, many individuals are using smart watches that can calculate their VO2max. Some of those smart watches, such as the Garmin forerunner 165, do a very good job of this, coming close to the measurements one would get in a laboratory, the Gold Standard. For instance, Firstbeat analytics, a company that provides physiological analytics and metrics for the Garmin watch, which is primarily geared toward athletes and based in Finland (Pitchbook, 2025), is a type of machine learning (ML) tool that can measure key biomarkers needed to calculate a more comprehensive biomarker, the VO2max. For instance, Firstbeat correlates exercise training variables and biomarkers such as heart rate, speed, velocity or speed changes, hill grade, as well as gender and age, into a number representing the individual’s VO2max. All this data becomes more meaningful and thus more accurate over time in predicting the individual’s VO2max.
But there is a glitch in what is out in the market presently regarding user-friendly smart watches, and who could really benefit. Although the best smart watch with the best analytics for measuring VO2max in endurance athletes, particularly runners, might be made by Garmin, the accuracy in measuring VO2max in the more sedentary or elderly individuals who are not going to be running is questionable at best. From my vantage point, I see that more effort needs to be put forth for these demographics by creating algorithms that will be needed not only for potentially pedestrian-like walking speeds, but also for activities of daily living and resistance training, so that all this information can be utilized to predict a VO2max number. Predicting VO2max based solely on running speed and grade variables is easy. The hard part is predicting a VO2max number based on these more nuanced variables.
But the future of smart watch technology should hold promise for the elderly as a more intelligent way of analyzing data is added. While traditional AI excelled at finding patterns and correlations (i.e., a greater increase in ice cream sales in July is correlated with a higher amount great white shark sightings), causal AI will go further to understand why things happen (i.e., Why are there more great white shark sightings in July? What is the cause?). This added layer of AI allows for a more intelligent way of arriving at the answer (AIthority, 2025), and in a fraction of time it would take a human. This translates over to the consumer, attaining more useful information that would also be beneficial for the more progressive doctors to know.
For instance, instead of the smart watch informing an individual their heart rate variability (HRV) has dropped, it could inform them why it has dropped. For instance, maybe there was a decrease in deep sleep combined with a rise in resting HR following a specific medication change perhaps. This distinction is crucial for understanding the pathophysiology, allowing doctors to pinpoint the true drivers of disease progression or health deterioration, not just associated symptoms (Mehta, Pranjal, 2025). Further, instead of just predicting an outcome, such as an 80% chance of heart failure, causal AI will help determine what intervention will have the desired effect (If the patient increases physical activity by X, the heart failure risk will be reduced by Y). All this information will help in going in the right direction, improving the key biomarker, VO2max.
BB
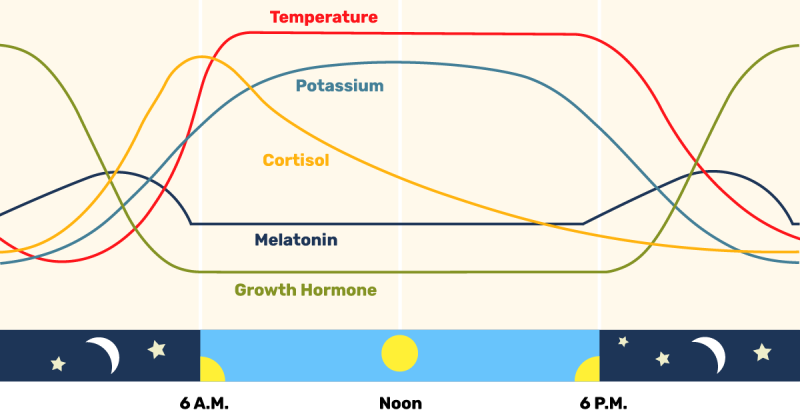
Figure 1a. Circadian Rhythm corresponding to hormone release.
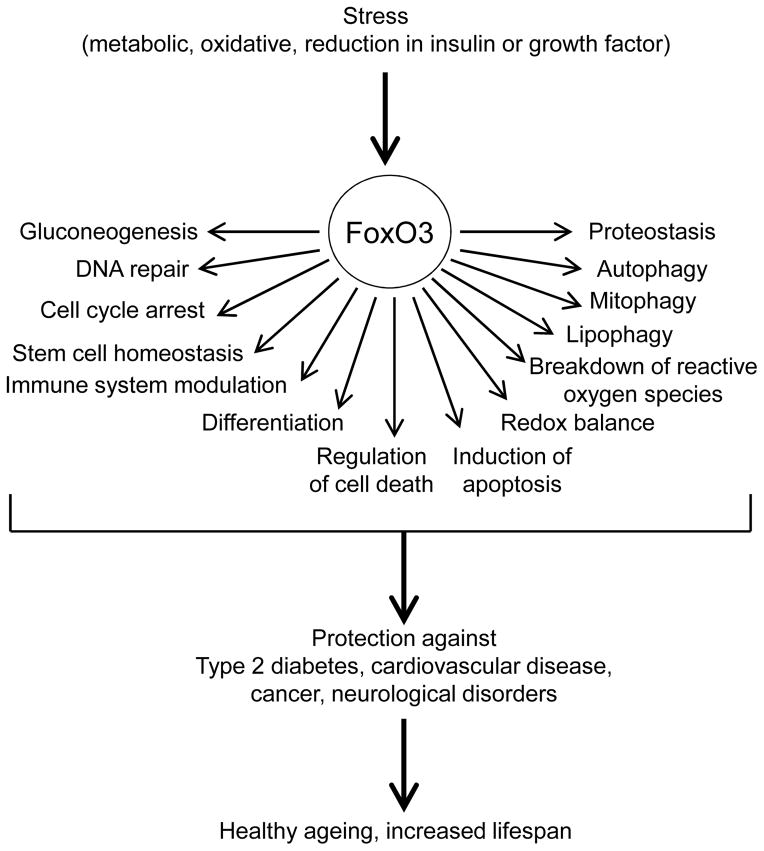
Figure 1b. There is an inverse relationship between IGF-1 receptor signaling and FOXO3 gene. When signaling is low, the FOXO3 gene is activated.
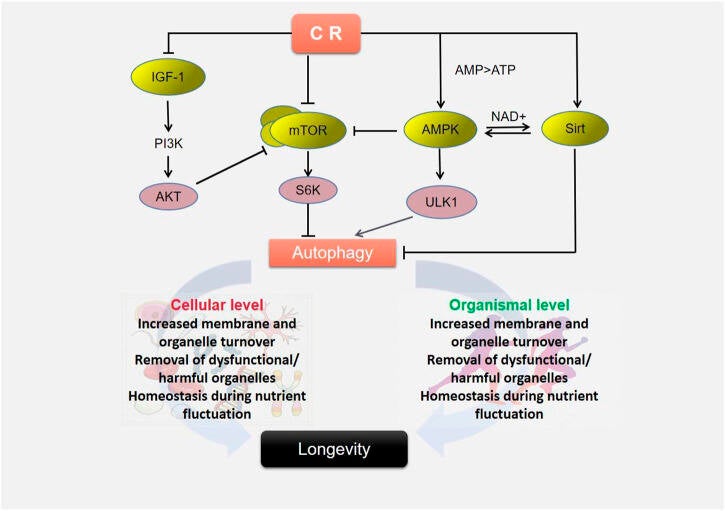
Figure 5a. Restricting calories can also lower IGF-1 levels.
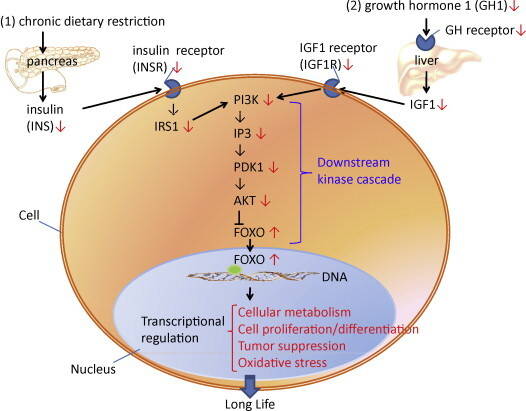
Figure 5b. Comprehensive overview of the inverse relationship between IGF-1 signaling and the FOXO3 gene.
VII. Circadian Rhythm and Blood Pressure Regulation
The sleep-wake cycle, or circadian rhythm is regulated on three levels: a core molecular level, an environmental level, and an autonomic level (Ruan, 2021). The three layers work together as a synchronized hierarchical system. The core molecular clock is in almost every cell of the body, operating on a roughly 24-hour negative feedback loop cycle, with the suprachiasmatic nucleus (SCN) of the brain acting as the master clock, synchronizing all peripheral clocks throughout the body to work as a unit; environmental signals act as time givers, aligning the molecular clock with the outside world; and, with communication from the SCN, the autonomic nervous system (ANS) executes the sleep-wake decision, adjusting body temperature and heart rate accordingly. But as an individual ages and the development of co-morbidities increase, a disturbance in the body’s circadian rhythm can potentially become disrupted, causing elevated nocturnal blood pressure, or reverse dipping that is fueled by the ANS’s sympathetic dominance, which can lead to the hastening of cardiovascular disease. This can also be seen with any individual with chronically poor lifestyle choices. In contrast, a healthy individual typically has a dip in blood pressure at night that is driven by the ANS’s parasympathetic dominance, and reinforced by the decrease in sunlight, which triggers key hormones to facilitate the sleep state. Upon awakening, the sympathetic nervous system’s (SNS) dominance increases blood pressure, known as the morning surge, reinforced by the increase in sunlight, which triggers key hormones to facilitate the wake state.
Yet an individual who leads a very healthy lifestyle could still struggle with chronic hypertension. This could also lead to nocturnal reverse dipping due to genetic reasons, such as an alteration in the DNA sequence or genetic variant, causing its overactivation (Kim, 2023). In time, this adversely affects renal and arterial functioning, causing molecular changes that affect cellular signaling and impaired tissue function. Eventually, systemic physiological imbalances occur, causing the increased blood pressure at night. In contrast, there are some ethnic groups that are resistant to an increase in blood pressure or reverse dipping at night, despite external environmental triggers that are generally not consistent in a 24-hour cycle, but instead, vary from day to day, or week to week. By studying their unique biomarkers and understanding what makes them tick genetically, we could adjust not necessarily our genetics, but instead, epigenetics or gene regulation through key lifestyle changes, and, hopefully, come closer to mimicking their physical traits or phenotypes.
- Molecular and Cellular Foundations
The Sunlight Trigger
Circadian rhythm exists in almost all life forms (Menezes-Junior, 2025) and regulates many physiological functions, from metabolism to immune response, renal function to sleep-wake-cycle, and the focus here specifically, blood pressure. Deregulation of the circadian clock can lead to hypertension. Sunlight plays an important role in this rhythm, triggering certain hormones as the sun rises, and triggering others as the sun’s light dissipates, preparing our bodies for sleep. As the sun rises, dopamine, serotonin, and cortisol are released, boosting mood, focus, and energy; as the sun diminishes, melatonin is released, promoting sleep (see figure 1a., Antosiek, 2026)
Looking at this on a grander scale, when morning sunlight hits the retina, a signal is sent through the retinohypothalamic tract of the retina to the SCN in the hypothalamus, synchronizing its rhythm to the environment. The SCN acts as the body’s master or central clock by synchronizing biological processes to Earth’s 24-hour light-dark cycle. In contrast, peripheral clocks are located throughout the rest of the body, in nearly every cell type. While external signals such as light and food synchronize and influence the central clock to the repetitive rhythm of the external stimuli, the central clock in turn influences the synchronization of the various peripheral clocks (Menezes-Junior, 2025).
This light-driven cycle controls circadian proteins, creating a feedback loop that exists inside the SCN cells. Key proteins that initiate a healthy negative feedback loop are the activators known as Circadian Locomotor Output Cycles Kaput (CLOCK), Brain and Muscle ARNT-like 1 (BMAL1), and the repressors known as three period genes (PER1-3), and two Cryptochrome genes (CRY1-2). The circadian cycle normally takes 24 hours to complete. The protein products of BMAL1 heterodimerize with those of CLOCK in the cell’s cytoplasm, then move to the nucleus, where together the CLOCK: BMAL1 heterodimer binds to specific DNA sequences called E-box enhancer elements in the promoters of target genes, such as PERs and CRYs (Faraci, 2025). The protein products of the PER and CRY genes, the “repressor team”, accumulate and re-enter the nucleus, where they inhibit the CLOCK: BMAL1 complex, the “activator team”, dampening their own transcription. This negative feedback loop can start again once PER and CRY concentrations have dropped.
A Genetic Enzyme Variant That Causes Disease
But this negative feedback loop can be thrown off course by a key mutation. According to Yang, et al (Yang, 2015), G protein-coupled receptors (GPCRs) are a large family of cell surface proteins that act as key messengers, allowing a cell to detect a wide array of signals from its external environment. Upon receiving these diverse signals, GPCRs trigger a series of events inside the cell that ultimately lead to a physiological response. In short, it changes the cell’s behavior. However, an enzyme that regulates GPCR function, G protein-coupled receptor kinase (GRK), when working abnormally, is involved in the pathogenesis of hypertension. There are seven GRK subtypes. Studies have found that hypertensive patients with the GRK4 variant are more likely to be non-dippers (lacking the drop in blood pressure at night) than those with the normal GRK gene. GRK4 is expressed in a few key organs such as the brain, kidney and vascular system that are all important in long term blood pressure regulation and control (Cao, 2021).
Looking deeper into the GRK4 gene, there is a genetic change in the DNA sequence that alters the corresponding amino acid in this protein. There are three key non-synonymous variants (R65L, A142V, and A486V), each one changing a specific amino acid at a particular position. These GRK4 variants have been associated with hypertension because they alter the function of the GRK4 protein in regulating blood pressure (Sanada, 2017). For instance, A142V polymorphism can produce high kinase activity, in that GRK4 phosphorylates GPCRs even without the typical upstream activation signal.
In any event, the GRK4 variant is permanently switched on and overactive, which prevents the PER/CRY repressors from successfully translocating into the nucleus at the correct time, thus they cannot turn off the CLOCK-MAL1 activators. The activators continue running, and the body in turn behaves as though it is still morning, even at night (Cao, 2020). As a result of the uncontrolled cycle, the kidneys are not properly excreting sodium during the night, the increased action of RAS causes vessels to constrict excessively, and the clock disruption prevents blood pressure from naturally dropping at night.
A Genetic Enzyme Variant That Promotes Longevity
In contrast, there is an ethnic group originating from Eastern Europe, specifically female Ashkenazi Jews of female gender and of shorter than average stature throughout life (2.5 cm below average height) who have mutations in their insulin-like growth factor (IGF-1) receptor gene. This gene mutation appears to restrict cell growth but extends human longevity (Scott, 2008). Although there is not necessarily a direct biological or genetic link to the characters mentioned in The Old Testament, present day Ashkenazi Jews are often referred to as having the “Methuselah Gene” due to their connection with longevity. As referenced in the Bible, Methuselah lived for 969 years (Genesis 5:21-27). Whereas the general population living to 100 years of age today is still a rare phenotype, with a prevalence of 1 in 10,000 individuals, in Ashkenazi Jewish women of short stature, the prevalence is much higher. Although the IGF-1 receptor gene is the focal point for analysis, there is a problem with measuring this concentration in centenarians, as there is less IGF-1 pathway activity in humans in general as they age. IGF-1 is produced by the liver in response to growth hormone (GH) released by the pituitary gland. GH drops roughly 14% per decade after age 30. By the time an individual is100, there is very little AGF-1 receptor produced, as there is very little GH released – a key reason these individuals live that long in the first place. Thus, the place to look is in the centenarian’s offspring, and analyze their IGF-1 levels (Suh, 2008).
In comparison to control groups, the female offspring of centenarians were found to be about 2.5 cm shorter than the female control groups, had a higher prevalence of the specific IGF-1R genetic mutations found in the centenarians compared to the control groups, leading to lower IGF-1 signaling, which all ultimately lead to greater longevity, even in cases where a less than stellar lifestyle existed, such as sleeping patterns that would adversely affect the general population, but not this segment of the population. In essence, reduced IGF-1 signaling is believed to protect carriers from cancer, cardiovascular disease, and metabolic issues. When the IGF-1 signaling is functioning in expected manner in mammalian physiology, FOXO3 is inhibited through phosphorylation. But the activation of FOXO3 is very important in its ability to set the stage for greater longevity, particularly specific variants in the FOXO3 gene, namely rs4946935. This variant of FOXO3 is essentially a protein or transcription factor that acts as a master switch, turning certain genes on or off. When IGF-1 signaling is low, FOXO3’s key variant is not inhibited, allowing it to enter the nucleus, triggering the expression of genes involved in autophagy, DNA repair, and stress resistance. (See figure 1b., Morris, 2015).
As a key example, my partner, “V”, is 73 years old, has worked the night shift (11PM – 8:30 am) since the early 1990s as an Emergency Physician, 4 nights per week, on a rotating shift where each week presents with different working nights. On the nights that she works, her sleep is staggered throughout the day, which for most people would be completely impossible for longer than 1 month. At 5 feet, 2 inches, she is very strong, fit, and healthy, with great mobility, strength, and endurance. Her parents originated from eastern Europe in the 1920s, survived the concentration camps of World War II, and after liberation, eventually met each other and moved to the United States. They are of Ashkenazi Jewish ethnicity. “V’s” mother is currently 100 years old.
- Cellular and Tissue-Level Mechanisms
When the GRK4 variant is permanently switched on in vascular smooth muscle cells, long-term adverse effects on tissues occur, primarily by enhancing the expression and function of the angiotensin type 1 receptor (AT1R). With more receptors active, the signal from angiotensin II to squeeze and grow is amplified. When angiotensin II binds to an increased number of these receptors, a hyperactive signaling loop is triggered, forcing blood vessels to overproduce collagen and thicken their walls, initiating the vascular remodeling process. Elastic tissues are replaced with less flexible, stiff fibers, directly increasing arterial stiffness and as a result, raising blood pressure (Chen, 2015).
How does this affect the heart tissue?
When the GRK4 variant (142V version) is permanently switched on, this enhances the Renin-angiotensin system instead of stopping it. The function of the AT1R is enhanced, raising Ang II signaling, and as a result, causing blood vessels to constrict severely and producing salt retention, resulting in high blood pressure that makes the heart work harder. The constant growth of myocardial cells causes the walls to become abnormally thick, stiffer, and less efficient at pumping. This Ang II signaling promotes the activation of fibroblasts, leading to increased scar tissue formation in the myocardium, making it stiffer. This chronic AT1R activation caused by the variant, triggers inflammation and oxidative stress, ultimately leading to the death of myocardial cells (Bhullar, 2022).
How does this affect kidney tissue?
When the GRK4 variant is permanently switched on, this creates a “gain of function” mutation that essentially locks the kidney in a state of high blood pressure and salt retention by supercharging AT1R, thus amplifying the Ang II signal. This causes the inability of the kidney to do its job in creating homeostasis, causing its inflammation, and preventing it from self-cleaning. For instance, the permanently active GRK4 variant leads to an increased production and activity of AT1R in the renal proximal tubules of the kidney, causing the kidneys to reabsorb far too much sodium and water, reducing urine output, and as a result, promoting hypertension. The combination of constant AT1R activation and the reduction in blood flow promotes inflammation, scarring, and damage to the renal tubules. The GRK4 variant also prevents other receptors from doing their job in getting rid of excess salt. Thus, the kidney loses its ability to regulate its own sodium excretion (Yang, 2019).
- Organismal Physiology
Whether the cause of a disrupted circadian rhythm causing a reverse dipping blood pressure is due to genetic or lifestyle factors, the commonality is the dysregulation of the ANS, specifically an overactivation of the SNS at night and the desynchronization of central and peripheral clocks. Normally, a nocturnal BP dip is primarily due to increased parasympathetic activity and decreased sympathetic activity during sleep, leading to a decrease in blood pressure at night of 10 – 20% compared with daytime. However, in individuals with a reverse dipping pattern, this balance is disrupted, leading to increased SNS activity during the night, and as a result, increasing heart rate and systemic vascular resistance, thus elevating BP. Some underlying conditions that can predispose an individual to this imbalance in autonomic function can be seen among individuals with renal diseases, autonomic neuropathies, diabetes, sleep apnea, autonomic dysfunction, malignant hypertension, and secondary hypertension. Over time, the lack of normal nocturnal rest throughout the body ultimately impairs its ability to recover, leading to structural changes in the arteries, myocardial structural and functional changes, renal dysregulation of fluid and sodium, cerebral damage, and disrupted melatonin and cortisol secretion (Okamoto, 2008)
Heart structure and function changes
For instance, structurally, the heart dimensions seen on echocardiography in non, or reverse dippers are interrogated as abnormal, when the ambulatory blood pressure measurements throughout the 24-hour period could even be relatively normal during the day, but increased during sleep. There is an increase in the left ventricle thickness or left ventricle hypertrophy (LVH); left ventricular mass is increased; the left atrial dimension is increased; the aortic root diameter is increased; and there is interventricular wall thickness (wall between the left ventricle and right ventricle chambers). There is also an increase in white matter lesions in the brain. Functionally, there is preserved stroke volume and thus cardiac output, but there is a marked increase in systemic vascular resistance at night, increased incidences of stroke, and in time, increased cognitive impairment leading to dementia (Routledge, 2007).
Chronic Kidney Disease (CKD)
Chronic kidney disease presents as the inability to eliminate excess sodium, causing extracellular fluid volume to expand, resulting in volume overload. This cascade effect initiates as the progressive decline in renal function, diminishing the kidneys’ capacity for effective sodium excretion (Mallamaci, 2025). The volume overload or fluid excess because of the kidneys’ inability to do the job is a major contributor to elevated nocturnal blood pressure, disrupting the delicate homeostatic balance that regulates blood pressure. Vascularly, increased stiffness and endothelial dysfunction occur due to this volume overload, intensifying the cardiovascular risks associated with CKD, a vicious cycle.
Dyssynchronization between Core Clock Genes versus Peripheral Clock
There are other systemic effects. The body’s central pacemaker, SCN, located in the hypothalamus, acts as the body’s master pacemaker. It uses light signals from the eyes to coordinate CR across peripheral organs, by essentially synchronizing peripheral clocks in organs like the kidneys and heart. But whether through genetic mutations affecting core clock genes, or lifestyle factors affecting that mistimed light exposure from shift work, there is a misalignment between the central clocks and peripheral clocks. This misalignment leads to the loss of a coordinated, healthy BP rhythm.
Normally, the SCN regulates the rhythmic production of melatonin by the pineal gland. Melatonin promotes sleep mainly by acting on MT1 and MT2 receptors located in the SCN. MT1 inhibits firing of SCN neurons, and as a result, it directly contributes to the sleepy feeling produced by elevated nocturnal melatonin. On the other hand, MT2 facilitates the shifting of CR, which helps to re-set the body’s clock in response to environmental changes in the light-dark cycle (Doghramji, 2007). However, this negative feedback loop can be disrupted in many ways. For instance, a study in a cohort of patients with hypertension showed a lower ratio of night/day concentration of melatonin in non-dippers for diastolic BP than in dippers, suggesting disruptions in the CR of these patients. Further, there was found an inverse relationship between the excretion of melatonin metabolites in urine during the night and the presence of a non-dipping BP profile.
- Population-Level Insights.
Surveys suggest that there are up to 3% of the adult population that suffer from circadian rhythm sleep disorders (CRSD). Some individuals are affected only temporarily because of jet lag; others affected need some form of treatment to prevent adverse medical, psychological and social consequences (Kim, 2013). Interrogating further into different chronic disease states, approximately 16% of CKD patients exhibit a reverse dipping blood pressure pattern (Gumz, 2022). In patients with CHF or sleep apnea, sleep disorders are more common, affecting between 55%-85% of CHF patients. This strongly correlates with abnormal circadian rhythm patterns such as non-or reverse dipping (Li, 2025).
Approximately 50% to over 70% of patients with chronic reverse dipping have underlying sleep apnea. Most of those patients have obstructive sleep apnea (OSA), at roughly 75% to 90% of the total percent suffering from sleep apnea (Castanho, 2018). In fact, where nighttime blood pressure is higher than daytime pressures, this is the strongest indicator for OSA, regardless of other factors. Key overt observations noted that are associated with OSA is obesity, which causes obstruction to the airway. This is generally related to a higher body mass index (BMI) than is healthy. Middle-aged men are more prone to OSA than woman, and key contributors are HTN, type 2 diabetes, asthma or COPD, genetic conditions, including Down Syndrome.
OSA and Obesity
According to meta-analysis (Esmaelli, 2025), although obesity is a significant factor in OSA development and severity, a notable significant percentage of people with OSA have a normal or slightly overweight BMI, indicating that obesity is not the sole cause. But with obesity and lack of conditioning comes key anatomical changes that cause this susceptibility. For instance, increased adipose tissue deposits around the neck and pharynx decrease the available airway space. There is also a greater upper airway collapsibility during sleep in obese individuals. Where the fat is located will also play a role. For instance, central obesity, or fat around the stomach and trunk causes reduced lung volume, decreasing the normal downward pull on the trachea towards the feet during inhalation (caudal traction), thus making the airway more likely to collapse. Further, the deconditioning that can lead to obesity and the reduced activity that comes with that lifestyle can contribute to apnea.
In contrast, only about 1% to 10% of those patients with sleep apnea have central sleep apnea (CSA), which is often linked to CHF, atrial fibrillation, stroke and other neurological disorders, as well as certain inherited disorders. Central sleep apnea causes nighttime oxygen drops or hypoxia followed each cycle with jolts of stress or sympathetic activity. Each of these episodes trigger a high heart rate with high blood pressure, and as a result, an overworked heart. This combination of chronic stress with low oxygen shortens the heart’s electrical recovery time, thus eventually making it susceptible to arrhythmias such as atrial fibrillation (Perger, 2023). The atrial fibrillation is further worsened by the chronic high blood pressure.
- Translational and Clinical Relevance
Since patients with GRK4 variants frequently exhibit a non-dipping blood pressure pattern where nocturnal blood pressure is increased, allopathic treatments that work by normalizing circadian fluctuation and reduce high nighttime blood pressure by inhibiting the overactive GRK4 kinase and inhibiting the renin-angiotensin system could be implemented. For instance, the angiotensin II receptor blocker (ARB) candesartan has been shown to be effective in treating hypertension caused by GRK4 variants, as these variants increase AT1R expression and function, leading to reverse dipping (Cao, 2021).
Just as important as the medication taken is the actual timing of that medication taken. Since blood pressure increases at night, causing reverse dipping, decreasing nocturnal SNS overactivity could be a strategy. Studies show that administering antihypertensive medications at night that block the RAAS system such as ACE inhibitors or ARBs would be better than administering them in the morning (Liu, 2022).
However, implementing a more holistic lifestyle that would create a more balanced ANS would be an important first step. If a healthy eating regimen is not in place that includes plenty of fresh fruits and vegetables, nuts and seeds, grains and legumes, and possibly lean meats, with little to no total daily sodium, processed meats, starches, stimulants nor sedatives, it would be good to start there (DASH diet). Likewise with activity. If a regular regimen of physical activity is not practiced daily, one that addresses strength and muscle building, endurance and power, mobility and balance, all at a properly regressed level that is within one’s ability, it would be good to develop that base. Once those regimens are followed, and blood pressure through ambulatory means has shown to be still too high, whether during the day and/or at night, then allopathic treatment should be administered. But at least all options holistically have been explored. Further, the timing of certain activities will assist in the proper sleeping process. Exercising earlier in the day so that hormones secreted during exercise that could negatively affect a sound sleep, are not an issue. Cortisol and adrenaline are released during exercise, which increases alertness and heart rate; norepinephrine can suppress melatonin, delaying sleep. Putting aside items 2 hours before bed that emanate blue light, such as iPhones, televisions and laptops are also a good idea.
Going beyond the lifestyle used in treating hypertension, there are other lifestyle changes that could be adopted to simulate the genetic advantages observed in the Ashkenazi Jewish centenarians and their immediate offspring. For instance, since they exhibit lower IGF-1 levels, there are eating patterns that can produce similar IGF-1 levels. By consuming fewer daily calories without trudging into malnutrition, this voluntary caloric restriction (CR) suppresses IGF-1 and mTOR pathways, which in turn enhances cellular cleanup, or autophagy (See figure 5a., Zhai, 2023). This is another visual with the inclusion of the cellular nucleus (See figure 5b., Chung, 2010). Similarly, intermittent fasting will reduce insulin and IGF-1 levels. Further, by reducing overall protein intake, particularly red meat, other potential risk factors are mitigated. Another key factor in longevity is possessing a key variant of the apolipoprotein E (APOE). APOE essentially provides instructions for making a protein involved in transporting fats and cholesterol through the bloodstream and brain. While the APOE2 variant is protective against Alzheimer’s disease, the APOE4 variant increases the risk for Alzheimer’s disease. Although possessing one or the other variant is genetic, a proper lifestyle can mitigate possessing the damaging variant. For instance, focusing on a heart-healthy diet, keeping one’s body mass index (BMI) low, and increasing the habit of physical activity on a regular basis, any genetic risk factors (i.e., APOE4 variant) can also be mitigated. Likewise, both CR and physical exercise can signal adenosine monophosphate (AMPK), which detects low ATP levels. AMPK in turn stimulates glucose uptake, fatty acid oxidation, and mitochondrial biogenesis to produce more ATP. While AMPK is activated, it directly phosphorylates FOXO3, which helps to sustain cellular energy homeostasis (Kjobsted, 2018).
Unfortunately, when it is all said and done, studies have consistently shown that the longevity of mere mortals does not stack up to those lucky ones with the so-called methuselah gene, who have claimed to live to 112 or more (Bakalar, 2011) due to their glass of daily wine, specific Cuban cigar, dark chocolate, or hauling their groceries upstairs on a regular basis. Despite these and other nonsensical anecdotes heard throughout the years, there are actual reasons for the longevity of super centenarians, whether a healthy lifestyle is followed or not. There is reduced IGF-1 signaling, increasing the activation of the FOXO3 gene for proper cellular maintenance and repair. There is a healthier lipid profile, with a decrease in the bad cholesterol (LDL) and an increase in the good cholesterol (HDL) due to the APOE2 variant, thus positively affecting every organ system of the body. However, with CR or caloric restriction, physical activity on a regular basis, and restful sleep where any reverse dipping is properly addressed, disease development can be mitigated. If nothing else, a greater health-span can be acquired. The years spent relatively healthily can be sustained for longer than if healthy habits were not followed. To quote a movie where eugenics dictates social class: “There is no gene for the human spirit.” (Niccol, 1997).
BB